
Laparoscopic Cholecystectomy in Dhaka: What to Expect, Recovery Timeline and FAQs
Considering laparoscopic cholecystectomy Dhaka patients often face, this practical guide lays out what happens before, during and after the operation at Popular Medical College Hospital. You will find clear preoperative instructions, a day-by-day recovery timeline with red flags, realistic cost and logistics, and straightforward answers to the questions patients ask most.
Who is a candidate for laparoscopic cholecystectomy in Dhaka
Clear rule: the operation is offered when gallbladder disease is causing symptoms, complications, or carries a clear risk that outweighs conservative care. Laparoscopic cholecystectomy Dhaka surgeons evaluate symptoms, imaging, and overall fitness before recommending surgery — not every gallstone needs removal.
Typical indications and important caveats
- Symptomatic gallstones: recurrent biliary colic with correlated ultrasound findings.
- Acute or chronic cholecystitis: when pain, inflammation or repeated attacks cause functional impairment.
- Complications of stones: history of gallstone pancreatitis (after initial stabilization) or obstructive jaundice requiring coordinated care with endoscopy.
- Suspicious gallbladder lesions: some polyps or a calcified gallbladder (clinical concern for malignancy) warrant removal rather than surveillance.
Practical consideration: patients with prior upper abdominal surgery, high BMI, or advanced cardiac or pulmonary disease are not automatically excluded from minimally invasive cholecystectomy. These factors change planning: anticipate longer operative time, possible need for additional ports, preoperative optimization, or a planned multi-disciplinary approach with anesthesia and ICU backup.
Trade-off to understand: choosing the most economical option in Dhaka is tempting, but lower cost can mean less experienced teams or limited access to intraoperative imaging and endoscopy. For safe outcomes, prioritize a surgical team that can perform intraoperative cholangiography or arrange prompt ERCP if required — this is where laparoscopic gallbladder surgery Dhaka centers with hepatobiliary expertise differ from generic general surgical units.
Referral and what to bring: bring your abdominal ultrasound report, any MRCP or endoscopy notes, a list of medications (especially blood thinners), and recent blood tests. If you prefer a direct route, book a surgical consultation with Dr Murshidul Arefin via the clinic consultation page so imaging can be reviewed before the visit.
Common misunderstanding: patients often believe absence of frequent pain means no future risk. That is false when there are concerning findings like a large polyp or suspicious wall calcification — in those cases observation can be riskier than surgery. Conversely, many small, asymptomatic stones do not require removal.
Concrete example: A 50-year-old man from Gulshan with monthly biliary colic and ultrasound-proven stones was referred to Popular Medical College Hospital. Preoperative MRCP showed a clear bile duct; after an anesthesia assessment the team scheduled elective minimally invasive cholecystectomy with same-team access to ERCP if required — he had an uncomplicated procedure and brief recovery. This illustrates typical selection and local coordination for laparoscopic cholecystectomy Dhaka patients.
Preoperative preparation and tests before surgery at Popular Medical College Hospital
Practical priority: Popular Medical College Hospital focuses preoperative workup on preventing last minute cancellations and avoiding unnecessary delays while making sure the team is ready for intraoperative surprises. For anyone scheduled for laparoscopic cholecystectomy Dhaka, expect targeted tests, a short anesthesia evaluation, and clear medication instructions rather than a long, unfocused battery of investigations.
Core tests and why we order them
- Basic bloods: complete blood count and basic metabolic panel to check anemia, electrolytes and baseline organ function.
- Liver profile: bilirubin, ALT, AST and alkaline phosphatase to detect possible common bile duct obstruction that changes the plan.
- Coagulation screen: PT/INR and APTT when there is bleeding risk or when anticoagulants are used; crossmatch only if clinically indicated.
- Cardiac check: ECG for people over 45 or with cardiac history; further cardiology input if abnormal.
- Selective imaging: an MRCP is arranged only when liver tests or ultrasound suggest a retained duct stone or unclear anatomy, not routinely for every patient.
Judgment point: ordering MRCP for every case is common in some clinics but it adds cost and delays surgery. In practice, a normal ultrasound and normal bilirubin make clinically important common bile duct stones unlikely. Reserve MRCP for elevated bilirubin, duct dilation on ultrasound, prior pancreatitis, or unresolved jaundice.
Medication, diabetes and fasting – specific, actionable rules
- Antiplatelets and anticoagulants: stop aspirin or clopidogrel 5 to 7 days if surgeon and cardiologist agree. For warfarin we aim for INR below institutional threshold and coordinate temporary reversal or bridging as needed.
- Direct oral anticoagulants: hold for 48 to 72 hours before surgery depending on renal function; confirm timing with the anesthetist.
- Diabetes medications: skip oral hypoglycemics on the morning of surgery and follow specific insulin instructions from the anesthesia team to avoid hypoglycemia and hyperglycemia.
- Fasting: no solid food for 6 to 8 hours and clear fluids up to 2 hours preoperatively unless your anesthetist gives different instructions. Arrive 2 to 3 hours before the scheduled time for paperwork and monitoring.
Practical insight: bring prior ultrasound images on your phone or printed CD and an up to date medication list. That single step often prevents repeated imaging and speeds decision making, especially when the team must decide whether to arrange preoperative ERCP or intraoperative cholangiography.
Concrete Example: A 62 year old man on warfarin from Mirpur had symptomatic stones and an INR of 2.6. The team gave a brief reversal plan, repeated INR the next morning and proceeded when it normalized. MRCP was performed because his bilirubin remained raised; the coordinated approach avoided emergency surgery and allowed elective laparoscopic cholecystectomy Dhaka with endoscopy backup available the same week.
Bring recent blood results and imaging to your appointment and upload them to the clinic before the visit via the consultation page at consultation.
Next consideration: if you have heart disease, diabetes or are on blood thinners arrange the anesthesia assessment as soon as surgery is planned so optimization happens before the admission day rather than on the morning of surgery.
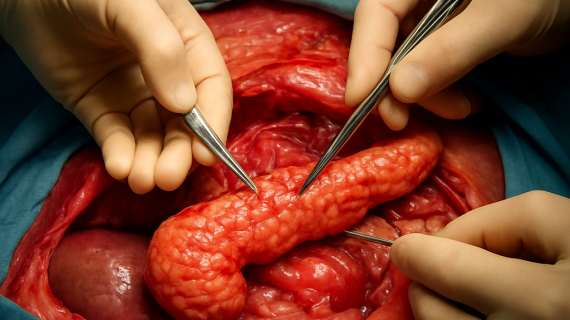
What happens during the laparoscopic cholecystectomy procedure
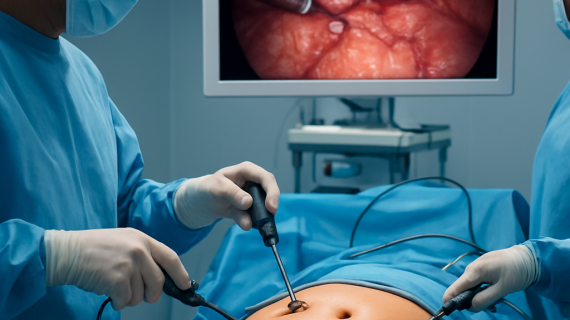
Immediate point: Laparoscopic cholecystectomy in Dhaka is performed under general anaesthesia in a dedicated laparoscopic operating theatre by a surgeon supported by an anaesthetist, scrub nurse and circulating staff — the team and equipment you see matter as much as the surgeon’s skill.
Main steps in the operating room
The operation follows a reproducible sequence designed to expose the biliary anatomy safely and remove the diseased gallbladder with minimal tissue trauma. Expect methodical, camera-guided work rather than hurried cutting.
- Anaesthesia and positioning: general anaesthesia with the patient tilted to improve exposure; antibiotic prophylaxis is given per protocol.
- Access: 3 to 4 small ports (keyhole incisions) are inserted and the abdomen expanded with carbon dioxide to create working space.
- Expose and clear: gentle dissection to reveal the cystic duct and cystic artery while protecting the common bile duct; the surgeon only proceeds once anatomy is clear.
- Secure structures: the cystic duct and artery are clipped and divided; if anatomy is uncertain the surgeon pauses and uses clarification techniques.
- Gallbladder removal: the organ is freed from the liver bed and extracted through a port, often in a retrieval bag to limit contamination.
- Final check and closure: irrigation if needed, ensure haemostasis, release the gas and close port sites carefully.
Practical insight: surgeons differ on routine use of intraoperative imaging. Intraoperative cholangiography helps detect unsuspected duct stones and clarifies anatomy, but it requires fluoroscopy and extends operative time; in practice at hepatobiliary centres in Dhaka it is used selectively when preoperative tests or intraoperative findings raise concern.
When conversion or additional procedures are needed
Conversion to an open incision is a surgical judgment, not a failure. Dense inflammation, unclear anatomy despite dissection, uncontrolled bleeding, or the need for a wider exploration are common reasons to convert. Choosing an early, controlled conversion is safer than persisting with forceful dissection that risks bile duct injury.
Trade-off to understand: advanced techniques like single-incision laparoscopy or energy devices can reduce visible scarring, but they increase technical difficulty and can lengthen surgery in difficult cases. For patient safety, most experienced hepatobiliary surgeons in Dhaka prefer the standard multiport technique for reliable exposure.
Concrete Example: At Popular Medical College Hospital a patient with an inflamed, fibrotic gallbladder had difficult dissection; the team used intraoperative cholangiography to confirm duct anatomy and then converted to a short right subcostal incision for safe removal. The controlled conversion avoided a bile duct injury and permitted rapid postoperative recovery.
Immediate recovery in theatre and the recovery room
After surgery you wake in recovery where staff monitor breathing, pain, and urine output. Pain is managed with short-acting opioids, non-opioid analgesics and sometimes regional blocks; nausea is treated promptly so oral fluids can begin when you are alert.
Next consideration: discuss the operative plan and contingency strategies at your preop visit so you understand when intraoperative cholangiography or conversion would be recommended — book a consultation via the clinic consultation page if you have specific concerns.
Risks, complications and how they are managed locally
Straightforward truth: laparoscopic cholecystectomy Dhaka is usually safe, but complications do occur and the important question is how quickly and effectively they can be identified and treated at your hospital.
How complications present and the practical local response
Minor problems: patients commonly have shoulder tip discomfort, nausea, and mild wound soreness after keyhole gallbladder surgery Dhaka. These are managed with simple measures — analytic laddering (paracetamol, NSAID, short opioid if needed), antiemetics, early mobilisation and outpatient wound care — and usually resolve in days.
Serious problems require systems, not luck. When unexpected bleeding, a bile leak, or obstructive jaundice appears, effective management hinges on rapid imaging, endoscopic access, and surgical judgment. That is why selecting a centre with on-site radiology, ERCP capability, and ICU backup matters more than the cheapest price.
- Practical pathway: if a patient develops fever and worsening abdominal pain after discharge the team will arrange urgent blood tests and an abdominal ultrasound; if fluid collection or bile leak is suspected, CT and interventional drainage are coordinated promptly.
- Endoscopy access: when retained duct stones or bile leak need treatment, ERCP with sphincterotomy and stent placement is the usual first-line intervention available at major Dhaka centres.
- Surgical escalation: uncontrolled bleeding, expanding abdominal collection, or unclear anatomy after initial surgery prompt either targeted reoperation or transfer to a hepatobiliary service with more resources.
| Complication | Usual initial sign | Local management pathway at a tertiary Dhaka centre |
|---|---|---|
| Wound infection | Redness, pus, localized pain | Oral/IV antibiotics, bedside opening and drainage; outpatient follow-up |
| Bile leak | Abdominal pain, persistent drain output, mild jaundice | Imaging → ERCP and stent; percutaneous drainage if collection present; surgery if not controlled |
| Post-op bleeding | Tachycardia, falling haemoglobin, abdominal distension | Resuscitation, urgent imaging, selective embolisation or reoperation depending on source |
Judgment you won't read everywhere: delayed recognition of a bile duct injury is the single biggest driver of long-term harm. In practice, choose a surgeon and hospital in Dhaka that will investigate any unexpected jaundice or persistent pain immediately rather than adopting a wait-and-see posture.
Concrete Example: A woman discharged the day after her laparoscopic operation returned with increasing abdominal pain and low-grade fever. Ultrasound at Popular Medical College Hospital showed a small subhepatic collection; the team placed a percutaneous drain and performed ERCP the next day to place a stent — she avoided reoperation and recovered in a week.
If you notice high fever, persistent vomiting, heavy wound bleeding, new yellowing of the eyes, or increasing abdominal pain after discharge contact your surgical team immediately or use the Popular Medical College Hospital emergency line via the contact page.
Detailed recovery timeline and aftercare plan
Direct point: recovery after a laparoscopic cholecystectomy Dhaka is largely predictable for uncomplicated cases, but safe, timely recovery depends on planning for pain control, wound care, and practical logistics — not just the operation itself.
Typical day-by-day course for an uncomplicated case
- Day 0 (day of surgery): monitored in the recovery area until awake and stable; early walking within hours, small sips of water once nausea settles, paracetamol/NSAID strategy started. Discharge that evening is common for fit patients who live close to the hospital and have a responsible companion.
- Days 1–3: expect gradually falling pain—take scheduled non-opioid analgesics, use short opioid course only if needed. Keep dressings clean and dry; gentle walks several times daily help reduce gas pain and constipation. Avoid driving while taking sedating pain medication.
- Days 4–14: most people resume normal light household tasks and desk work during this window. Increase walking and low-impact activity; avoid lifting objects heavier than about 10 kilograms. Watch for changes in bowel habit; transient loose stools are not unusual as your body adjusts to bile flow changes.
- Weeks 3–6: stamina and abdominal strength return slowly; full return to manual labor, heavy lifting or vigorous gym workouts is usually safe after 4–6 weeks with surgeon approval. If symptoms such as persistent bloating or new jaundice appear, re-evaluation is required.
Practical insight and trade-off: same-day discharge reduces cost and hospital-acquired risks but trades off immediate in-hospital observation. If you live more than an hour from Dhanmondi, have unreliable transport, or significant comorbidities (uncontrolled diabetes, cardiac disease), an overnight stay at the hospital is the safer choice.
Medication note: a multimodal plan (scheduled paracetamol and an NSAID, rescue short opioid, antiemetic PRN) controls most postoperative pain. Routine prolonged opioids are unnecessary and increase constipation and recovery delays — discuss a clear stop date with your surgeon before discharge.
Concrete Example: A 34-year-old bank officer from Banani had elective minimally invasive cholecystectomy and went home the same afternoon. She stopped opioids by day 2, returned to desk work on day 9, and avoided heavy lifting for four weeks; she used the clinic hotline when low-grade fever developed on day 3 and was reassured after a brief phone assessment.
- Two-week checklist: confirm follow-up appointment, remove remaining dressings as advised, continue wound observation for discharge or redness, maintain a stool softener if constipated, and note any persistent nausea or yellowing of eyes.
- When to delay discharge: uncontrolled pain despite meds, inability to tolerate fluids, or unstable vitals — these require observation or further tests.
Next consideration: arrange your first postoperative visit within 7 to 10 days and confirm emergency contact details before discharge so you have clear access to your laparoscopic surgeon in Dhaka if anything unexpected happens.
Cost, payment options and appointment logistics in Dhaka
Straight fact: final cost for a laparoscopic cholecystectomy Dhaka patients pay depends on more than the surgeon fee — theatre consumables, anaesthesia, imaging (or ERCP), and any unplanned escalation (conversion to open surgery or ICU care) drive most of the variation. Get an itemised estimate before you commit.
Typical cost components and realistic ranges
| Component | Typical range (Bangladeshi Taka, approximate) |
|---|---|
| Surgeon professional fee | 20,000 – 60,000 |
| Anaesthesia fee | 8,000 – 20,000 |
| Operating theatre, disposables and consumables | 30,000 – 90,000 |
| Room and nursing (1 night) | 6,000 – 20,000 |
| Additional imaging / ERCP if required | 10,000 – 80,000 |
| Total for an uncomplicated elective case | 70,000 – 220,000 |
Practical insight: that wide range exists for a reason. A straightforward elective procedure with clear anatomy stays near the lower end. If preoperative or intraoperative findings require ERCP, longer theatre time, implants, or a conversion to open surgery the bill rises quickly. Cheap initial quotes often exclude these contingencies.
- Accepted payment methods: cash, major credit/debit cards, bank transfer, and mobile banking — confirm what the hospital accepts before admission.
- Insurance and employer schemes: limited local private insurance exists; obtain preauthorization and a written estimate. Corporate or employer billing is possible but requires advance approval.
- Deposit and final billing: many Dhaka hospitals ask for a deposit to reserve theatre time; request a provisional invoice showing likely additional costs for ERCP, ICU or extra days.
Appointment logistics — what actually speeds things up: schedule your surgical consultation using the clinic page at consultation and upload your ultrasound, MRCP or prior notes in advance. Providing images and recent blood results before the visit prevents repeat testing and gives you a realistic cost estimate on the first visit.
Trade-off to decide: paying a bit more for a hepatobiliary-capable team in Dhanmondi gives you on-site ERCP, radiology and ICU backup. That costs more up front but reduces the chance of emergency transfer and higher downstream expense — in my experience this is the better value for patients with complicated anatomy or prior biliary problems.
Concrete Example: a patient from Uttara booked elective laparoscopic gallbladder surgery, paid a deposit of 25,000 taka and provided ultrasound images online. The operation was uncomplicated and final billing matched the estimate. A second patient required same-admission ERCP for a retained duct stone and the final bill rose accordingly — both outcomes show why you must budget for contingencies.
If scheduling matters, private-pay elective slots will be faster. If you prefer slower, lower-cost public options, expect longer wait times and verify what emergency services the facility provides.
Choosing a surgeon and why patients in Dhaka choose Dr Murshidul Arefin
Practical point: for laparoscopic cholecystectomy Dhaka patients, the surgeon is one part of a system. Experience matters, but what changes outcomes is access to a hepatobiliary team, timely imaging, and endoscopy (ERCP) on the same site. Pick a surgeon who operates within that system, not one who works alone and refers out for complications.
What to prioritise — beyond reputation
Key criteria: look for a laparoscopic surgeon in Dhaka with regular hepatobiliary case volume, demonstrable experience with difficult dissections and conversions, and documented collaboration with interventional endoscopy and radiology. High volume and multidisciplinary access reduce the chance that a complication becomes an emergency transfer.
- Team capability: can the hospital provide ERCP and CT/US on short notice?
- Outcome transparency: ask about local conversion and complication handling rather than general success claims
- Communication style: does the surgeon explain contingency plans clearly and in plain language?
- Logistics: proximity to Dhanmondi and admission flexibility for family support matter for early discharge decisions
Practical trade-off: cheaper quotes from clinics without on-site ERCP or ICU tempt patients who want lower upfront cost. In practice this is a false economy for anyone with prior pancreatitis, abnormal liver tests, or inflammation on ultrasound — managing a retained duct stone or bile leak is faster and cheaper when ERCP is available immediately.
Concrete example: a patient from Mohammadpur chose Dr Murshidul Arefin because Popular Medical College Hospital offered same-admission ERCP. During surgery an unexpected duct stone was suspected; the team performed intraoperative imaging and arranged ERCP the next morning without transfer. The coordinated approach avoided reoperation and shortened the total stay.
Judgment most patients overlook: surgical skill is necessary but not sufficient. The real safety margin is institutional – consistent theatre teams, experienced anaesthesia, immediate endoscopy, and senior radiology support. When choosing among top surgeons in Dhaka, prioritise the one embedded in a complete hepatobiliary service rather than the lowest fee.
- Questions to ask at your consultation: How many laparoscopic cholecystectomies do you perform monthly? What is your conversion policy when anatomy is unclear? Is ERCP available here and how quickly? What follow-up and emergency contact will I have after discharge?